Arguably the biggest problem faced by the Medical Officer of Health was death by disease, and one of the most important tasks the Medical Officer of Health was tasked with was recording the mortality rate succinctly in each report. Tracking deaths in a MOH’s district was crucial, which also coincided with the trend in the nineteenth century of the state becoming more interested in its peoples . By keeping detailed records of how many people had died for whatever reason meant that the spread or dissipation of particular diseases was noted, and therefore it could clearly be seen whether an epidemic was likely or not. Public health statistics, like overall mortality rates per annum or per quarter were also useful in that it was concrete evidence for higher classes to learn about one side of urban life they may not be familiar with.

Keeping note of mortality rates also had the benefit of clearly illustrating population. Drastic population increase had a knock-on effect to all the other issues Medical Officers of Health had to deal with. If there was overcrowding in particular areas, it meant there were unsanitary conditions, which in turn led to disease outbreaks. It was up to the Medical Officers of Health to decide whether mortality rates over a period of time were too high or just acceptable and unavoidable. Medical Officers of Health could do a number of things to try and appeal to the state for reform. Specific preventative health programmes could be suggested, or it may just be as general as advocacy for reform or better sanitary conditions. Disease in slum conditions was an inevitability, but death could be avoided.
The Public Health Act 1848 was instrumental in pushing for public health reform but also really began the work of Medical Officers of Health. The Act mean that building regulations and sanitation legislation were able to be put in place which could, in theory, help limit the spread of infectious disease like cholera. However, these small pushes for reform paved the way for modern public health: “resolutely counter-attacking the armies of disease and death.”
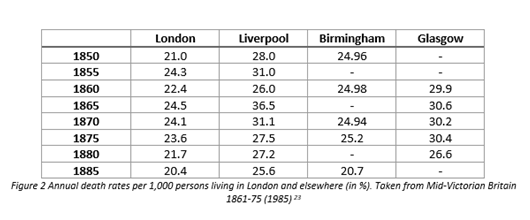

A table of mortality rate percentages and averages, like the one pictured above, were useful not only to a Medical Officer of Health, but is also useful for us in the present day and as historians. Quantitive data is always useful as a research tool. It helps historians have a more ‘scientific’ tool to help prove their hypothesis, instead of relying on other types of data. It means there is less need to rely on qualititative data which has its own setbacks and is an alternative to making assumptions based on first-hand accounts of any particular event. It is also useful as mortality rates are usually made up of a large sample size and so can be generalised far more broadly.
The first cholera outbreak in England occurred in Sunderland in 1832, a few years prior to the introduction to the introduction of the first Medical Officer of Health. Cholera quickly spread across the country and hit London. Over 16,000 people died in total in England and Wales as a result of cholera.
Cholera was dangerous, and spurred the state to take greater care into the welfare of slums and poorer areas of the country, as “the fear of cholera became a crucial element in the development of public health in Britain.” Cholera and disease was thought of only as a poor man’s disease. John Simon, the first Medical Officer of Health declared in his first report: “The frightful phenomenon of a periodic pestilence belongs only to defective sanitary arrangements.” Social reformers and also Medical Officers of Health pushed hard for state to take a role in the health of its citizens, and also proved how useful surveys and reports of general health and mortality rates were. Robert Baker in Leeds proved that high mortality rates, epidemic disease and working class areas went hand in hand. Cholera the disease that defined the Victorian era, and was thankfully almost completely eradicated by the turn of the century.
All disease could not be eradicated though, only quelled slightly to the best of the Medical Officer of Health’s ability, and that was still purely dependent on what funding they were allowed and how well they could state their case to local government that there was a serious problem that needed to be dealt with. That is not to say that the MOH was a null job, rather the work that they did manage to do was pioneering in itself though and without their work it can be argued that England and Wales would have been far worse off. The introduction of the Medical Officer of Health also demonstrates the development of a modern British welfare state, as welfare states tend to “reflect the dominant cultural and political characteristics of their societies.” The Victorian era was the perfect period for a welfare state to truly start flourishing, and the introduction of Medical Officer of Health thus proves that, as an increased state presence wherein social and economic matters could as a result flourish even further.
As Geoffrey Best summarised perfectly: “Their achievement was a great one, considering all the circumstances, of preventing the cities from becoming more lethal than they already were.”
